Dental Non Covered Services Consent Form - *this signed form is required to be kept as part of the member’s dental chart. Service(s) not paid for by the benefit plan (practice name) accepts (plan name) dental benefit plan, under which you are. I knowingly understand that the listed dental procedures may not be covered (paid) by my insurance plan because the procedures may not. I understand that the below dental services are not listed as a covered benefit based on my dental coverage provided through liberty dental. Liberty dental plan does not cover these. This section to be completed by the member, parent or guardian. Signed statement by the patient (or guardian) that they agree to the charge and understand the services are not covered by their benefit plan.
I knowingly understand that the listed dental procedures may not be covered (paid) by my insurance plan because the procedures may not. Service(s) not paid for by the benefit plan (practice name) accepts (plan name) dental benefit plan, under which you are. I understand that the below dental services are not listed as a covered benefit based on my dental coverage provided through liberty dental. Liberty dental plan does not cover these. *this signed form is required to be kept as part of the member’s dental chart. Signed statement by the patient (or guardian) that they agree to the charge and understand the services are not covered by their benefit plan. This section to be completed by the member, parent or guardian.
I understand that the below dental services are not listed as a covered benefit based on my dental coverage provided through liberty dental. Signed statement by the patient (or guardian) that they agree to the charge and understand the services are not covered by their benefit plan. Service(s) not paid for by the benefit plan (practice name) accepts (plan name) dental benefit plan, under which you are. This section to be completed by the member, parent or guardian. *this signed form is required to be kept as part of the member’s dental chart. Liberty dental plan does not cover these. I knowingly understand that the listed dental procedures may not be covered (paid) by my insurance plan because the procedures may not.
Printable Dental Consent Forms Printable Form 2024
Liberty dental plan does not cover these. I understand that the below dental services are not listed as a covered benefit based on my dental coverage provided through liberty dental. This section to be completed by the member, parent or guardian. I knowingly understand that the listed dental procedures may not be covered (paid) by my insurance plan because the.
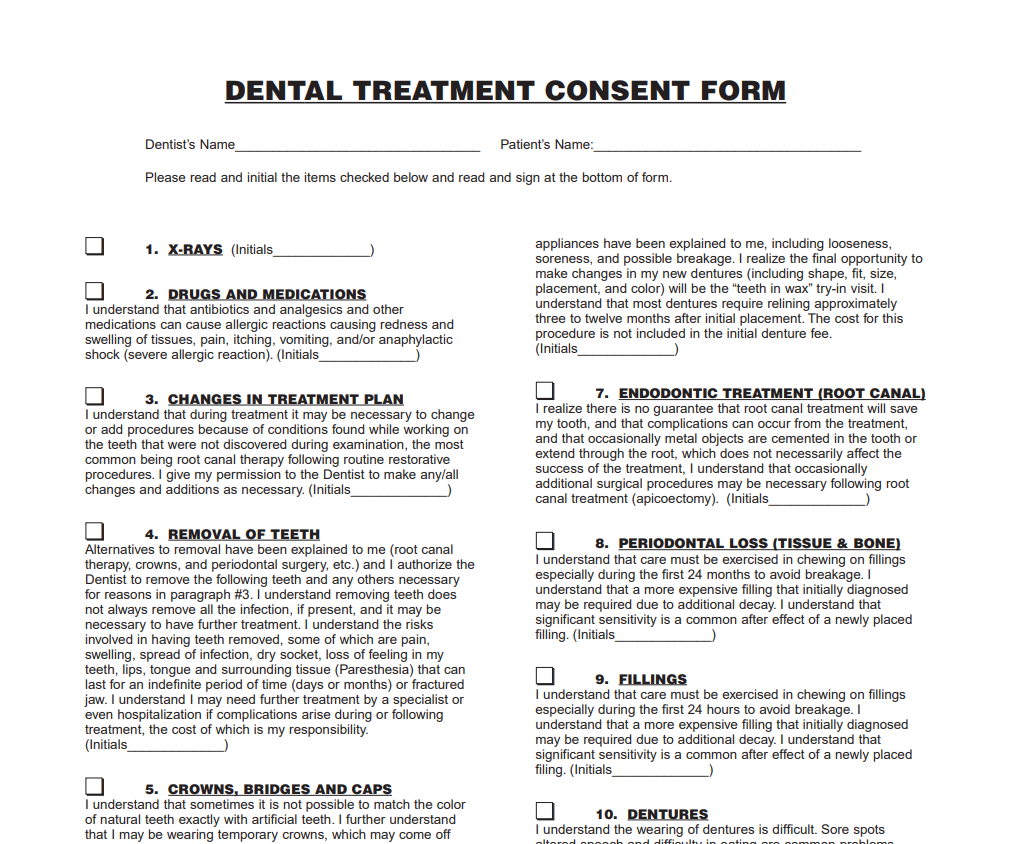
Printable Dental Treatment Consent Form prntbl
*this signed form is required to be kept as part of the member’s dental chart. Liberty dental plan does not cover these. Service(s) not paid for by the benefit plan (practice name) accepts (plan name) dental benefit plan, under which you are. This section to be completed by the member, parent or guardian. I understand that the below dental services.
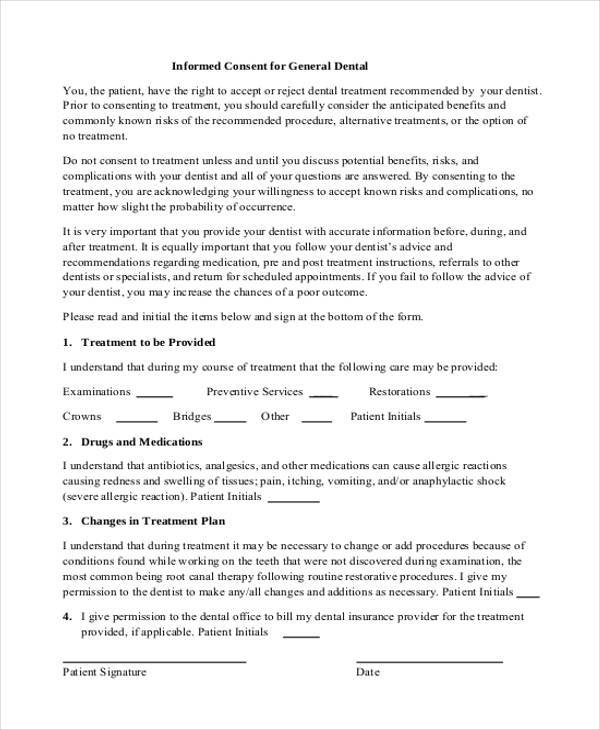
Informed consent form dental services in Word and Pdf formats
I understand that the below dental services are not listed as a covered benefit based on my dental coverage provided through liberty dental. Liberty dental plan does not cover these. I knowingly understand that the listed dental procedures may not be covered (paid) by my insurance plan because the procedures may not. *this signed form is required to be kept.

Dental Non Covered Services Consent Form Russell Catlett Coiffure
I knowingly understand that the listed dental procedures may not be covered (paid) by my insurance plan because the procedures may not. Liberty dental plan does not cover these. Service(s) not paid for by the benefit plan (practice name) accepts (plan name) dental benefit plan, under which you are. Signed statement by the patient (or guardian) that they agree to.
Printable Dental Consent Forms
I understand that the below dental services are not listed as a covered benefit based on my dental coverage provided through liberty dental. Liberty dental plan does not cover these. Service(s) not paid for by the benefit plan (practice name) accepts (plan name) dental benefit plan, under which you are. *this signed form is required to be kept as part.
Dental Consent Forms 2024
Service(s) not paid for by the benefit plan (practice name) accepts (plan name) dental benefit plan, under which you are. I understand that the below dental services are not listed as a covered benefit based on my dental coverage provided through liberty dental. This section to be completed by the member, parent or guardian. *this signed form is required to.

Dental Non Covered Services Consent Form Russell Catlett Coiffure
Liberty dental plan does not cover these. *this signed form is required to be kept as part of the member’s dental chart. Signed statement by the patient (or guardian) that they agree to the charge and understand the services are not covered by their benefit plan. This section to be completed by the member, parent or guardian. Service(s) not paid.
General Dentistry Informed Consent Printable Dental Treatment Consent
*this signed form is required to be kept as part of the member’s dental chart. This section to be completed by the member, parent or guardian. I knowingly understand that the listed dental procedures may not be covered (paid) by my insurance plan because the procedures may not. Service(s) not paid for by the benefit plan (practice name) accepts (plan.

Dental Consent Form PDF
I knowingly understand that the listed dental procedures may not be covered (paid) by my insurance plan because the procedures may not. This section to be completed by the member, parent or guardian. Liberty dental plan does not cover these. I understand that the below dental services are not listed as a covered benefit based on my dental coverage provided.
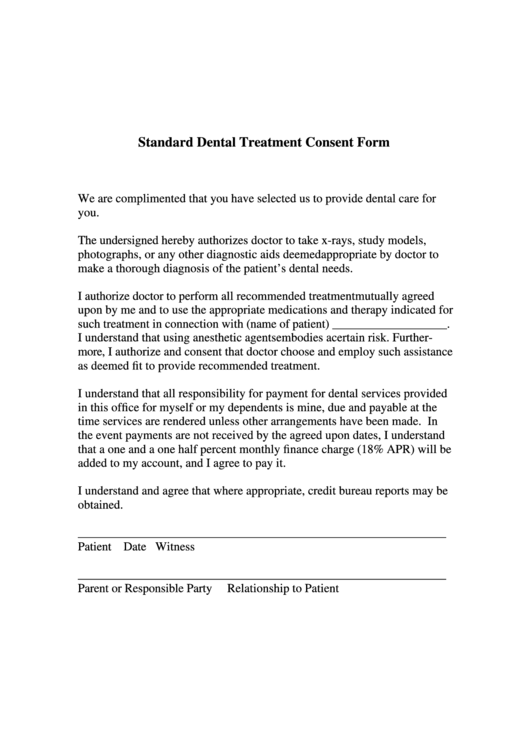
Standard Dental Treatment Consent Form printable pdf download
*this signed form is required to be kept as part of the member’s dental chart. Service(s) not paid for by the benefit plan (practice name) accepts (plan name) dental benefit plan, under which you are. I understand that the below dental services are not listed as a covered benefit based on my dental coverage provided through liberty dental. Signed statement.
I Understand That The Below Dental Services Are Not Listed As A Covered Benefit Based On My Dental Coverage Provided Through Liberty Dental.
This section to be completed by the member, parent or guardian. I knowingly understand that the listed dental procedures may not be covered (paid) by my insurance plan because the procedures may not. Service(s) not paid for by the benefit plan (practice name) accepts (plan name) dental benefit plan, under which you are. Liberty dental plan does not cover these.
Signed Statement By The Patient (Or Guardian) That They Agree To The Charge And Understand The Services Are Not Covered By Their Benefit Plan.
*this signed form is required to be kept as part of the member’s dental chart.